One of my most recent cases was a patient with a tri-malleolar fracture due a slip on ice. Due to this time of the year, in the lovely northeast, I would like to go over some details about how a simple slip on ice can lead to an injury that requires surgical intervention.
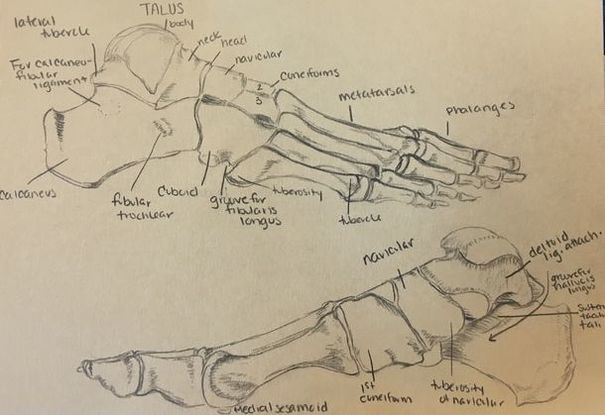
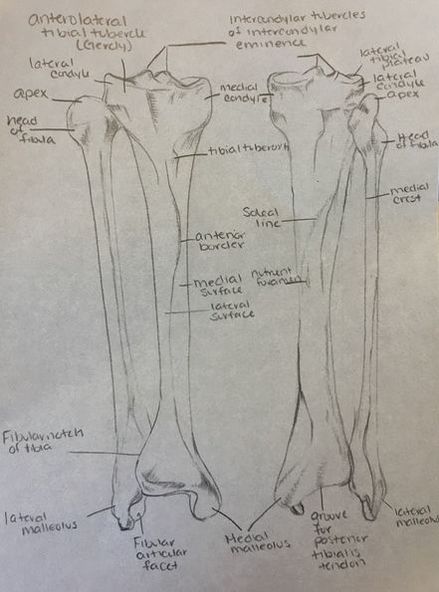
Below are photos up that I drew just for some basic anatomy of the foot and leg.
Below are photos up that I drew just for some basic anatomy of the foot and leg.
Lets say a 54 year old female presents to your urgent care with some ankle pain after her fall on the ice. She is wheeled into the clinic as she states that she cannot walk on her foot. After getting details of her fall and note that she cannot bear weight on it since the fall, you start your physical exam. You inspect her ankle and note significant ecchymosis (bruising), maybe even some around her calcaneus. She has limited ROM due to pain with flexion and extension of her ankle and is extremely tender to touch on both medial and lateral malleoli. She is not tender on the dorsum, metatarsals, or navicular region of her foot.
Before getting x-rays remember the OTTAWA Ankle Rules to determine if x-rays are needed:
Before getting x-rays remember the OTTAWA Ankle Rules to determine if x-rays are needed:
- Unable to bear weight or walk >4 steps in the clinic/ER
- Ankle films needed
- Pain along lateral malleolus
- Pain along medial malleolus
- Foot films needed
- Midfoot pain
- 5th metatarsal pain or navicular pain
| Bimalleolar Ankle Fracture In this type of injury, there is a fracture to the medial malleolus as well as lateral malleolus. Upon visit to ER or clinic the patient will likely have to have it reduced (which means realigned into place), then splinted. Typically, during an acute injury, they use splints as opposed to casts to allow for soft tissue swelling. Unfortunately, these types of injuries do not heal well anatomically on their own and require surgical intervention. During surgery, the surgeon will reduce the fracture as much as possible and anatomically align the bones before placing screws and a plate to keep the bones aligned during healing. The patient usually will keep these screws and plate in their ankle for the rest of their life as long as there is not discomfort with them after the fractures are fully healed. Everyone heals at their own rate, but usually this will take about 6-8 weeks to 3-4 months to heal well to the point where the patient can return to most daily activities. It will take up to a year for the patient to feel like they did prior to the injury. |  Bimalleolar fracture (left) ORIF with plate and screws (right) For more graphic photos Google "bimalleolar fracture ORIF" Photo above from nursingcenter.com Trimalleolar Ankle Fracture To make this a "tri" the same injury can occur but the distal posterior aspect of the tibia (posterior malleolus) is also fractured or avulsed. As my preceptor was explaining, he does not put a screw in that fracture as it will heal while the others are stabilized. |
Weber Ankle Fracture
This fracture has different classifications depending on how many ligaments are involved. A Mortise view of the ankle is best used for diagnosis along with clinical examination.
Weber A *Every ligament is intact with a fibular fracture*
Tibiofibular syndesmosis is intact (attachments of distal fibula to distal tibia).
Deltoid ligament intact (attaches medial malleolus to the calcaneus, talus, and navicular bones)
Fracture of fibula below Mortise (talotibial joint line)
Typically stable and does not require surgery
Weber B *Fracture of fibula is at the same level of Mortise*
Tibiofibular syndesmosis is intact maybe a mild tear
Deltoid ligament intact or maybe torn
Fracture of fibula at the same level of Mortise
Can be stable or unstable (if unstable requires ORIF)
Weber C *Widened talofibular joint with fx above Mortise*
Tibiofibular syndesmosis is torn causing widened talofibular joint
Deltoid ligament torn ± medial malleolus fracture
Fracture of fibula above Mortise
Unstable and requires ORIF
This fracture has different classifications depending on how many ligaments are involved. A Mortise view of the ankle is best used for diagnosis along with clinical examination.
Weber A *Every ligament is intact with a fibular fracture*
Tibiofibular syndesmosis is intact (attachments of distal fibula to distal tibia).
Deltoid ligament intact (attaches medial malleolus to the calcaneus, talus, and navicular bones)
Fracture of fibula below Mortise (talotibial joint line)
Typically stable and does not require surgery
Weber B *Fracture of fibula is at the same level of Mortise*
Tibiofibular syndesmosis is intact maybe a mild tear
Deltoid ligament intact or maybe torn
Fracture of fibula at the same level of Mortise
Can be stable or unstable (if unstable requires ORIF)
Weber C *Widened talofibular joint with fx above Mortise*
Tibiofibular syndesmosis is torn causing widened talofibular joint
Deltoid ligament torn ± medial malleolus fracture
Fracture of fibula above Mortise
Unstable and requires ORIF
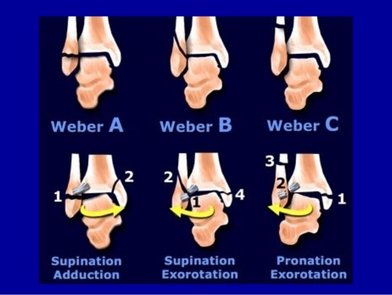
Photo from an awesome slideshow on Slide Share http://www.slideshare.net/drhawler1/ankle-injury-amanj
Common Ankle Sprains
Note that regardless of the type of Weber, the Anterior Talofibular Ligament is intact, this is the ligament that attaches the lateral malleolus to the talus. ATFL is most commonly torn/sprained with ankle inversion injuries (think of twisting your ankle with the sole of your foot turning inward). Other ligaments in the lateral ankle complex are the calcaneofibular ligament and posterior talofibular ligament.
If you were to sprain your ankle with an eversion injury (turning the sole of your foot outward), this would likely injure the deltoid ligament which, as stated above, attaches the medial malleolus to the medial foot). There are 4 ligaments that make up the deltoid ligament (posterior tibiotalar, anterior tibiotalar, tibiocalcaneal, and tibionavicular) the names are easy to remember if you remember where the the ligaments are attaching.
Grades of Ankle Sprains
I. Ligament stretched but intact (able to bear weight, and do normal activities)
II. Partial ligament tear (difficult to bear weight, able to do activities but with extreme pain)
III. Complete tear/rupture of the ligament (unable to bear weight)
Note that regardless of the type of Weber, the Anterior Talofibular Ligament is intact, this is the ligament that attaches the lateral malleolus to the talus. ATFL is most commonly torn/sprained with ankle inversion injuries (think of twisting your ankle with the sole of your foot turning inward). Other ligaments in the lateral ankle complex are the calcaneofibular ligament and posterior talofibular ligament.
If you were to sprain your ankle with an eversion injury (turning the sole of your foot outward), this would likely injure the deltoid ligament which, as stated above, attaches the medial malleolus to the medial foot). There are 4 ligaments that make up the deltoid ligament (posterior tibiotalar, anterior tibiotalar, tibiocalcaneal, and tibionavicular) the names are easy to remember if you remember where the the ligaments are attaching.
Grades of Ankle Sprains
I. Ligament stretched but intact (able to bear weight, and do normal activities)
II. Partial ligament tear (difficult to bear weight, able to do activities but with extreme pain)
III. Complete tear/rupture of the ligament (unable to bear weight)



