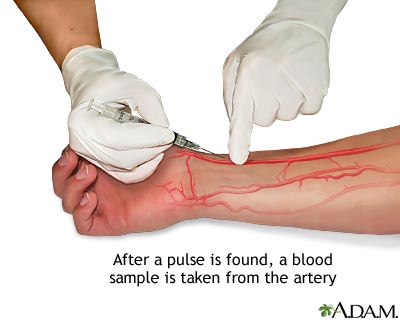
In clinical skills lab, we get to learn all the fun, hands-on things we will get to do as PA's. Today, we got to practice ABG's (Arterial Blood Gases) and splinting. Now, I have drawn hundreds and hundreds, maybe even near a thousand patients, but I have never done an ABG. The difference between an ABG and simple blood draws is that an ABG is arterial blood. The blood drawn for those colorful tubes and that IV giving you medications, is all venous blood. An ABG has to be performed by a professional either a provider or respiratory therapist because more things can go wrong when obtaining blood from an artery than a vein. That being said, today we practiced these ABG's on a simulation arm that had "blood" pulsating through it. Below you can see a picture of the radial artery being used for an ABG. Typically, this is the artery of choice. The way we can tell if we are locating an artery in contrast to a vein is that it will pulsate AND the blood will be brighter in color (that is, as long as the patient is not completely hypoxic). Unlike regular routine blood draws from veins (that have thinner more flexible walls), during an ABG the needle is held at a much greater angle (about 45-90 degrees) upon puncture. The ABG is then put on ice and sent to the lab where the pH, bicarbonate, PaCO2, PaO2 and %O2 levels are measured. With this blood gas we can tell if a patient is in respiratory acidosis, metabolic acidosis or neither. Typically, if the body is in respiratory acidosis the rest of the body will respond with compensated metabolic alkalosis (more basic in order to make up for the acidity that the lungs are creating due to a low respiratory rate, retaining too much CO2 or other issues). Since gas exchange in the lungs happens with every breath at many alveoli and capillaries, the respiratory response is much faster (minutes to hours) than the metabolic response (hours to days). The reverse can happen as well, where the body is in metabolic acidosis and then the lungs can compensate and cause respiratory alkalosis. A variety of these acid/base combinations can occur and cause the body harm; therefore, measuring these levels will help providers understand what the patient needs in order to get better.
After the ABG practice, we learned how to properly splint fractures, sprains and dislocations! I have been waiting for this since day 1 in January. With simple little cases our instructor presented to us, we looked at x-rays and determined what kinds of splints helped the best with different fractures. I have helped many PA's and MD's in the ER with splinting and always wondered how they knew what type of splint to make especially when there were so many fractures or maybe even just a sprain! Even if someone presents to the ER with what looks like a sprain, clear x-ray and some swelling--- splint them and refer them to ortho! Splinting typically allows for some acute swelling so when the patient goes to their orthopedic they can protect their injury until then without completely restricting their blood flow (or worse! cause compartment syndrome). As we practiced each case, we slowly became a little better and less messy with the plaster/wrapping. I seem to have a tough time with keeping the bulk to a minimum, but I will keep practicing! Below is a picture of what an awesome job my partner did on my splints! Great work Jeff!




