As I stated before, every Friday we are tested on our skills for various physical exams. The past two Fridays we focused on EENT. Starting with the ear, nose, and throat exam we learned how to exam the external and middle ear as well as perform simple hearing tests. That week's exam I was chosen, again, to perform my skills. I felt very lost looking in my partner's ear canal at first because this was something I never did before...I didn't want to hurt my partner by sticking the otoscope too far in her ear! Surprisingly, I was able to see the TM (tympanic membrane), cone of light and malleus very clearly on my first try. What I was seeing through the otoscope can be seen in the image on the left. The focus of this view is the TM. The malleus is the long thin bone extending from the center of the TM to the top right. The cone of light is the light reflection slightly right of the center on the TM.
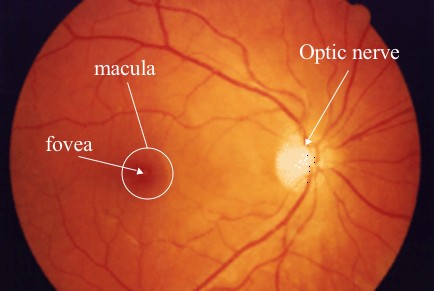
This Friday we focused on the eye exam. We tested for visual acuity, the vital sign of the eye, extraocular movements, and examined the optic disk, fovea and macula. In the picture on the top right you can see what the retina looks like inside the eye. This is the type of view we get from the ophthalmoscope. Here the white round disc on the right is the optic disc, essentially where the optic nerve (CN II, the cranial nerve responsible for vision) connects to the eye. If a patient has papilledema the disc will look different and distorted. This condition is caused from increased cranial pressure. Patients will often report having a headache and see changes in their visual field as well as decreased visual acuity; however, papilledema can also be asymptomatic before any vision loss occurs. If left untreated, patients can lose their vision completely. In patients with glaucoma, the optic disc will look enlarged and much brighter white because there is an increase in intraocular pressure due to the decrease in drainage of aqueous humor in the anterior chamber of the eye. This condition is often genetic and much more common in those with darker eyes. Even though this seems like it would be painful, a patient will not notice this change because it happens gradually over time. Many patients with glaucoma have regularly scheduled visits to their ophthalmologist to have their intraocular pressures checked. Unfortunately, glaucoma is irreversible but the progression of the condition can be delayed with proper medications.
The macula and fovea can only really be seen when the patient is looking directly into the light. This is because in this part of the eye there are the most cones which can see color and detail very well.
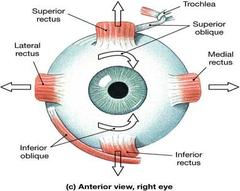
The extraocular movements were tested by having the patient follow my finger in an H pattern to test all of these muscles attached to the eye. Surprisingly there are three different cranial nerves that are responsible for moving the eye around (CN III, IV, VI).
Hopefully, that wasn't too much medical jargon for some of you reading this blog, but I feel like typing all this out really helps me study as well as teach some readers a thing or two!
This Friday we focused on the eye exam. We tested for visual acuity, the vital sign of the eye, extraocular movements, and examined the optic disk, fovea and macula. In the picture on the top right you can see what the retina looks like inside the eye. This is the type of view we get from the ophthalmoscope. Here the white round disc on the right is the optic disc, essentially where the optic nerve (CN II, the cranial nerve responsible for vision) connects to the eye. If a patient has papilledema the disc will look different and distorted. This condition is caused from increased cranial pressure. Patients will often report having a headache and see changes in their visual field as well as decreased visual acuity; however, papilledema can also be asymptomatic before any vision loss occurs. If left untreated, patients can lose their vision completely. In patients with glaucoma, the optic disc will look enlarged and much brighter white because there is an increase in intraocular pressure due to the decrease in drainage of aqueous humor in the anterior chamber of the eye. This condition is often genetic and much more common in those with darker eyes. Even though this seems like it would be painful, a patient will not notice this change because it happens gradually over time. Many patients with glaucoma have regularly scheduled visits to their ophthalmologist to have their intraocular pressures checked. Unfortunately, glaucoma is irreversible but the progression of the condition can be delayed with proper medications.
The macula and fovea can only really be seen when the patient is looking directly into the light. This is because in this part of the eye there are the most cones which can see color and detail very well.
The extraocular movements were tested by having the patient follow my finger in an H pattern to test all of these muscles attached to the eye. Surprisingly there are three different cranial nerves that are responsible for moving the eye around (CN III, IV, VI).
Hopefully, that wasn't too much medical jargon for some of you reading this blog, but I feel like typing all this out really helps me study as well as teach some readers a thing or two!
 |   |



